Case: An 18 year old female with a past medical history of anxiety, 2 weeks post-op from tonsillectomy presents for chest pain. She woke up today with severe, non-radiating central chest pain. Her daily medications include sertraline and oral contraceptives. Vitals are BP 118/86, HR 119, Temp 97.7F, RR 24, SpO2 96% on room air. On exam, she is uncomfortable appearing and tearful. Her oropharynx is clear without signs of erythema or drainage. She is tachycardic without murmurs and has clear lung sounds bilaterally. There are no signs of lower extremity swelling. EKG and point-of-care cardiac ultrasound are shown below:
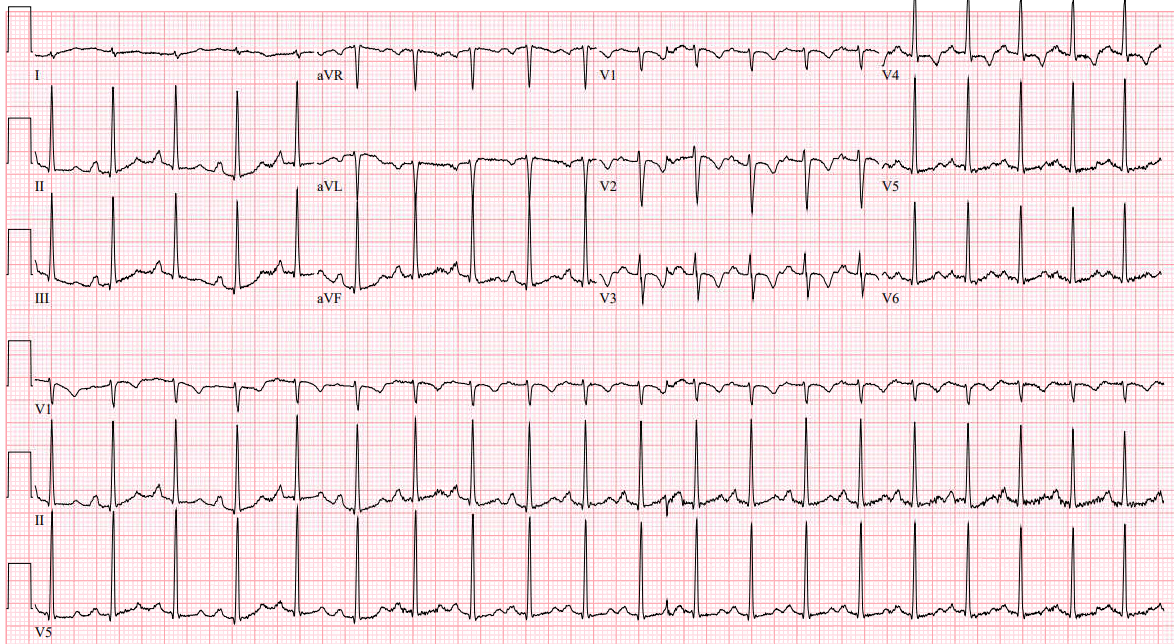
EKG interpretation: Sinus tachycardia with rightward axis and T wave inversions in anterior leads
POCUS interpretation: Normal LV ejection fraction. No pericardial effusion. Elevated RV to LV ratio. Dilated IVC with < 50% collapse with inspiration. RV free wall hypokinesis with apical hyperkinesis. Tricuspid annular plane systolic excursion 1.0 cm.
Case continued: Due to high concern for pulmonary embolism, the patient is empirically started on heparin. CTA chest results with acute pulmonary embolism with right heart strain. High sensitivity troponin results markedly elevated at 306 mg/dL. Patient is admitted to the ICU with interventional cardiology consultation. Patient underwent pulmonary arteriogram which demonstrated elevated PA pressures without need for thrombectomy and was discharged in good condition on hospital day #4.
Pearls:
- Infants and toddlers can have normal T wave inversions in the anterior leads known as “juvenile T waves” which should turn upright by age 7.
- Any T wave inversion in these leads after they have flipped upright is abnormal.
- While the S1Q3T3 EKG finding is classically associated with pulmonary embolism, more common EKG findings suggestive of PE include sinus tachycardia, rightward axis, incomplete right bundle branch block, and T wave inversions in the anterior leads.
- Empirically start anticoagulation in patients with high concern for pulmonary embolism prior to definitive imaging.
- Right ventricular free wall hypokinesis with apical hyperkinesis is known as McConnell’s sign and is pathognomonic for acute pulmonary embolism.
- Other POCUS findings include an RV:LV ratio > 1 which is sensitive but not specific. A tricuspid annular plane systolic excursion (TAPSE) < 17 mm is a quantitative measure to diagnose right heart dysfunction on echocardiogram.
References:
Kline JA. Venous Thromboembolism Including Pulmonary Embolism. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw Hill; 2020.
Goodacre, S., & McLeod, K. (2002). ABC of clinical electrocardiography: Paediatric electrocardiography. BMJ (Clinical research ed.), 324(7350), 1382–1385. https://doi.org/10.1136/bmj.324.7350.1382
Alerhand S, Hickey SM. Tricuspid Annular Plane Systolic Excursion (TAPSE) for Risk Stratification and Prognostication of Patients with Pulmonary Embolism. J Emerg Med. 2020;58(3):449-456. doi:10.1016/j.jemermed.2019.09.017